

"Just rest, give it some time, and let’s see how it feels in a few weeks."
For decades, traditional physical therapy relied on this exact formula: subjective feedback, visual observation, and manual touch. But while a seasoned clinician's intuition is invaluable, the human eye has its limits. A runner's subtle asymmetry at mid-stance or an athlete’s hidden deficit in eccentric braking force after an ACL reconstruction can easily go undetected.
Today, physical therapy looks completely different.
The profession has undergone a massive evolution, transitioning from a bachelor’s or master’s credential to a rigorous Doctorate of Physical Therapy (DPT). Modern PTs are autonomous primary practitioners deeply trained in complex biomechanics and clinical research.
This high-level clinical education has opened the door to a new era of sports medicine that replaces guesswork with objective, evidence-based data. Guessing isn't good enough.
Our guiding mantra is simple: Don’t Guess, Test.
By integrating state-of-the-art diagnostic technology directly into our daily clinical workflow, we are turning subjective observations into precise, quantifiable data. Here is how modern technology is redefining rehabilitation and performance.
1. Dual Force Plates: Measuring Impact & Asymmetries
Force Plates, at the root of it, are just really expensive bathroom scales. But from those “bathroom scales” we can derive a litany of data points that the human eye alone cannot detect:

Force
Velocity
Impulse
Rate of Force Development
Eccentric Braking Force
Peak Power
The Bottom Line: Force plates provide an objective roadmap of how an athlete handles impact and where they are compensating. This data allows for targeted rehabilitation, helping to correct imbalances before they lead to re-injury.
2. Digital Dynamometers: Precision Strength Profiling
Traditional strength testing relies on a clinician pushing against a patient’s limb and guessing strength on a subjective 1-to-5 scale. While fine for spotting major nerve damage, it fails to capture the subtle strength gaps that hold an athlete back from full recovery.

Digital dynamometers solve this by isolating specific muscle groups to measure exact force down to the pound or kilogram. Whether checking a soccer player's hamstring-to-quad ratio or a pitcher's shoulder rotation, it replaces guesswork with cold, hard data.
The Bottom Line: By comparing exact numbers against the uninjured limb or healthy averages, clinicians know precisely when a muscle is fully recovered.
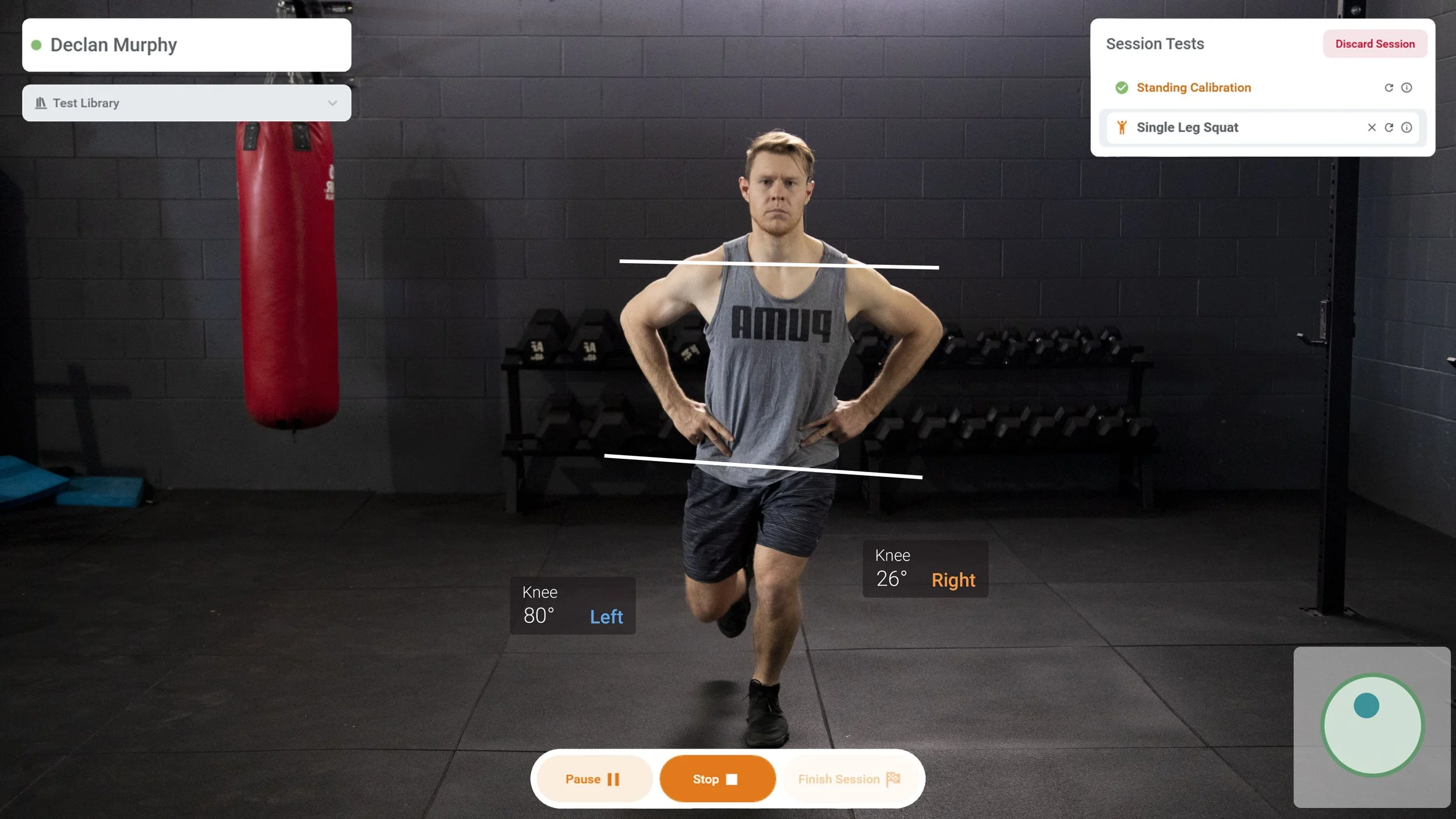
3. 3D Motion Capture & Biomechanical Analysis
The human eye can see the general movement but might lack the acuity to determine minute asymmetry.
3D motion capture changes the game by digitizing human movement. By breaking down joint rotation, pelvic tilt, and trunk lean frame by frame, we can pinpoint exact "energy leaks" and mechanical flaws that drive chronic overuse injuries like tendonitis.
Furthermore, the data is clear: systematic reviews show that objective biomechanical assessments are essential for predicting injury risk and safely clearing competitive athletes for return-to-sport (1). If you can't measure it, you can't fix it.
Breaking Through Plateaus: Fear and Progress Monitoring
Data alone is just numbers but in the hands of an expert clinician, it is a powerful physical and psychological tool.
Injuries don’t just happen to the body; they happen to the mind. One of the biggest roadblocks in rehab is fear. Hesitation and fear can cause athletes to hit plateaus and delay their return to play.
Data can help dismantle this fear. Seeing objective proof that their quad strength or jump force is steadily improving builds cognitive confidence. It proves to their brain that their body is resilient and capable.
It proves they are not made of glass.
Furthermore, clinicians should never rely on a "trust me, it's working" approach. If the data shows an athlete isn't progressing after weeks of training then the plan isn't working. It forces the clinician to stop guessing, pivot, and find a better path forward.
Criteria vs. Time: The Flaw of the Ticking Clock
Traditionally, rehab is bound to a calendar: "You are four months post-op, so you are cleared to run."
But a ticking clock is a terrible metric for biological readiness. Every athlete has a unique injury history, different performance goals, distinct genetics, and highly individualized healing timelines. Clearing someone based entirely on time completely ignores their actual physical capacity.
We must transition to criteria-based return-to-play. We shouldn't care what the calendar says; we should care what the data say about an athlete's actual physical abilities.(10)
ACL Rehab as an Example
For decades, the "gold standard" for clearing an athlete after an ACL reconstruction has relied on functional hop tests. Clinicians compare the injured leg to the uninjured leg to calculate a Limb Symmetry Index (LSI). If the injured leg scores above 90% compared to the healthy one, the athlete is cleared.
The Failure Rate: Despite hitting this 90% benchmark, ACL re-tear rates have stubbornly remained around 30% for decades(7).
Why the System is Failing:
Good Tools, Bad Strategy: Hop tests aren't useless, they are great for observing overall movement and coordination. The issue is relying on them as the only gatekeeper for return-to-sport clearance.
Outdated Excuses: Historically, clinics used tape measures and stopwatches because advanced laboratory equipment was too expensive. Today, sophisticated diagnostic technology is affordable, compact, and accessible to any clinic.
Hidden Deficits: Research proves that standard LSI calculations mask true deficits and overestimate a knee's actual stability and function. (9)
Athletes Want to Win: Athletes can easily "cheat" a distance test by using their hips or ankles to compensate for a weak knee or quad. (4,5)
The Bottom Line: Relying strictly on low-tech distance testing creates a false sense of security, failing to predict long-term athletic success or protect athletes from re-injury.
The New Standard
In a world of biohacking and health wearables, it’s only logical that physical therapy step up and take advantage of technology. By combining doctorate-level clinical reasoning with sophisticated tech, we can look beneath the surface. We can ensure an athlete isn't just moving, but moving safely and efficicently.
Stop letting a calendar dictate your health, and stop relying on visual guesswork. Armed with the right tools and the right knowledge, it's time to make truly objective decisions. It’s time to start testing. Schedule a consultation and discover the difference objective, evidence-based care can make.
Bibliography
Alahaidib, A., Alyousef, H., Sharif, M., Alsulaiman, A., Alharthi, T., Aljohani, H., Almutairi, M., Alghamdi, N., Almutairi, K., Alammari, A., & Almehizia, A. (2025). Biomechanical Assessment Tools for Injury Risk Prediction and Return-to-Sport Evaluation in Athletes: A Systematic Review. Cureus, 17. https://doi.org/10.7759/cureus.93210
Gill, V., Tummala, S., Sullivan, G., Han, W., Haglin, J., Marks, L., & Tokish, J. (2024). Functional Return-to-Sport Testing Demonstrates Poor Predictive Value of Long-Term Outcomes Following ACL Reconstruction: A Systematic Review. Arthroscopy: The Journal of Arthroscopic & Related Surgery. https://doi.org/10.1016/j.arthro.2023.12.032
Hart, C., & Chumanov, E. (2025). Investigation of Force Plate Jump Testing Metrics Relevant to Return to Play Decision Making in Basketball Athletes After Anterior Cruciate Ligament Reconstruction. International Journal of Sports Physical Therapy, 20, 985 - 994. https://doi.org/10.26603/001c.141101
Kotsifaki, R., Sideris, V., King, E., Bahr, R., & Whiteley, R. (2023). Performance and symmetry measures during vertical jump testing at return to sport after ACL reconstruction. British Journal of Sports Medicine, 57, 1304 - 1310. https://doi.org/10.1136/bjsports-2022-106588
Kotsifaki, A., Van Rossom, S., Whiteley, R., Korakakis, V., Bahr, R., Sideris, V., & Jonkers, I. (2022). Single leg vertical jump performance identifies knee function deficits at return to sport after ACL reconstruction in male athletes. British Journal of Sports Medicine, 56, 490 - 498. https://doi.org/10.1136/bjsports-2021-104692
Robles-Palazón, F., Comfort, P., Ripley, N., Herrington, L., Bramah, C., & McMahon, J. (2023). Force plate methodologies applied to injury profiling and rehabilitation in sport: A scoping review protocol. PLOS ONE, 18. https://doi.org/10.1371/journal.pone.0292487
Rodriguez-Merchan, E. C., & Valentino, L. A. (2022). Return to Sport Activities and Risk of Reinjury Following Primary Anterior Cruciate Ligament Reconstruction. The archives of bone and joint surgery, 10(8), 648–660. https://doi.org/10.22038/ABJS.2021.50463.2504
Smiley, T., Dallman, J., Long, R., Kapple, M., Aldag, L., Mok, A., Bernard, C., Martin, K., Vopat, L., & Vopat, B. (2024). Lower extremity return to sport testing: A systematic review. The Knee, 50, 115-146. https://doi.org/10.1016/j.knee.2024.07.021
Wellsandt, E., Failla, M., & Snyder-Mackler, L. (2017). Limb Symmetry Indexes Can Overestimate Knee Function After Anterior Cruciate Ligament Injury. The Journal of Orthopaedic and Sports Physical Therapy, 47(5), 334-338. https://doi.org/10.2519/jospt.2017.7285
Winkler, P., Thorolfsson, B., Piussi, R., Snaebjörnsson, T., Senorski, R., Karlsson, J., Samuelsson, K., & Senorski, H. (2025). Sport-specific concomitant injuries, return-to-sport rates and second anterior cruciate ligament (ACL) injuries in adolescents with ACL reconstruction. British Journal of Sports Medicine, 59. https://doi.org/10.1136/bjsports-2024-108694