
Radial nerve entrapment, also known as Radial Tunnel Syndrome, is a condition in which the radial nerve that runs along the bones and muscles of the elbow and forearm is compressed. Compression or entrapment can occur at any location along the path of the nerve, but the most frequent location occurs in the proximal forearm, near the elbow.
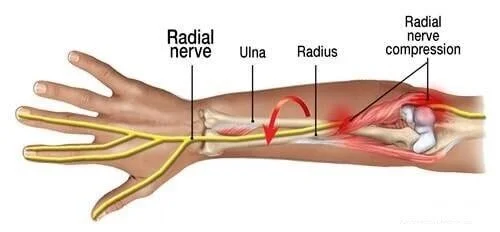
Image courtesy of www.diseasesdic.com
Symptoms typically develop slowly and can include pain, weakness, or paresthesias (abnormal sensation like numbness, or tingling). This condition can often be confused with lateral epicondylitis, or “tennis elbow” since lateral elbow pain can be a symptom of both lateral epicondylosis or radial tunnel syndrome.

Image courtesy of Thieme
The radial nerve originates in the brachial plexus with nerve roots C5-C8 and T1. In other words, it comes from nerves exiting the cervical spine that merge in the shoulder to form the nerves of the arm.
It travels down the back of the upper arm, between the medial and lateral heads of the triceps. It then pierces the intermuscular septum, and crosses the outer elbow passing between the brachialis and brachioradialis in the radial tunnel to the front of the lateral epicondyle. It then divides into branches that travel down into the forearm and hand.
The radial nerve innervates, or stimulates, the following muscles: triceps, brachioradialis, brachialis, and extensor carpi radialis longus. It predominantly gives sensation to the back of the arm, forearm, and hand.
Radial nerve entrapment is often thought to be a result of overuse, but it does occur due to other causes - such as direct trauma, fractures, compressive devices, or post-surgical changes. Most commonly it occurs in patients who participate in recreational (e.g., sports) and occupational activities with repetitive motions such as pushing or pulling, twisting, gripping with the hand or bending the wrist.
Overuse of these motions can lead to compression and/or traction at mobile or stable joints, while direct trauma can cause sudden inflammation and changes to the surrounding tissue. Prolonged local swelling and edema can result in partial or complete nerve damage if it is not addressed. Recovery of function is more likely with a mild injury, thus a shorter duration of compression. Recovery is faster if the repetitive activities that exacerbate the injury can be decreased or ceased.
As with most injuries, there are varying degrees of nerve damage severity. In mild cases, the compression of the nerve causes no permanent damage and the nerve fully recovers. For some, the nerve injury may require more intervention than conservative care alone. A recent study from 2018 evaluated the efficacy of a single corticosteroid injection in radial tunnel syndrome, finding improved outcome measures in 57% of subjects at 1 year follow-up (Marchese et al). More severe cases, with permanent damage to the nerve from partial or complete laceration, can cause persistent deficits that may need to be addressed surgically.
To learn more, check out these articles and texts:
Marchese, J., Coyle, K., Cote, M., & Wolf, J. M. (2019). Prospective Evaluation of a Single Corticosteroid Injection in Radial Tunnel Syndrome. HAND, 14(6), 741–745. https://doi.org/10.1177/1558944718787282
Radial Nerve Entrapment. Buchanan, B.K.; Maini, K.; Varacallo M. Copyright © 2020, StatPearls Publishing LLC. Bookshelf ID: NBK431097 PMID: 28613749. http://creativecommons.org/licenses/by/4.0/
Am Fam Physician. 2010;81(2):147-155. Copyright © 2010 American Academy of Family Physicians.
American Journal of Roentgenology. 2010 Sept;195(3): 585-594. doi: 10.2214/AJR.10.4817. https://www.ajronline.org/doi/full/10.2214/AJR.10.4817